Case 11: Closure of a larger defect on the cheek with the versatile bilobed flap
Sahar Vanessa Amiri (MD) and Matilda Svenning Hunt (MD)
Published · April 2, 2025
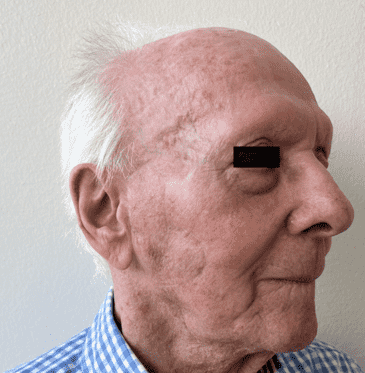
Keywords: bilobed flap, larger facial skin defects, cheek reconstruction, reconstructive surgery Authors: Sahar Vanessa Amiri (MD) and Matilda Svenning Hunt (MD). Institution: Department of Plastic Surgery and Burns, Rigshospitalet, Denmark Abstract This case describes the use of a bilobed flap for reconstruction of a large cheek defect following excision of a squamous cell carcinoma in an 86-year-old male. Due to the tumor size and previous surgical scarring, direct closure was not feasible. The bilobed flap was chosen as the preferred reconstructive approach because of its ability to provide adequate coverage of the defect while allowing for primary closure of the donor site. Postoperative follow-up at three months demonstrated satisfactory aesthetic outcomes, with no wound complications or recurrence. Patient medical history The patient, an 86-year-old male diagnosed with hypertension, paroxysmal heart flutter, and with a history of carcinoma, was referred to us with a large, localized tumor on the right cheek. According to the patient's history, the tumor had been present for more than one year. The biopsy showed squamous cell carcinoma, and the histological subtype was unspecified. On clinical examination, the tumor was described as 20*25*6 mm, localized on the parotid gland, and clinically not adherent to the underlying tissue. The patient had a scar from a previous full-thickness skin graft (FTSG) on the right temple. There were no palpable regional lymph nodes. The patient was operated on under local anesthesia. Because of the size of the tumor, direct closure was not feasible. Local flaps were deemed a preferred reconstruction method. The tumor was excised with a 7 mm safety margin and depth excision margin to SMAS (Superficial Musculoaponeurotic System). Histology from frozen sections showed no malignancy. Before and After Patient examination The patient presented with significant sun damage and poor skin quality. The tumor was 20 x 25 mm in diameter and e
Step-by-step
- Step 1
- Step 2
- Step 3
- Step 4
References
- Steele, R. , Jellinek, N. , Foy, A. , Lee, K. , Vij, A. & Knackstedt, T. (2020). Use of Ex-tranasal Bilobed Transposition Flaps in Cutaneous Reconstructive Surgery at 2 Institu-tions. Dermatologic Surgery, 46 (10), 1279-1285. doi: 10.1097/DSS.0000000000002319.
- Lal T, Lal J. Bilobed Flaps: An Esthetic Method of Reconstructing Circular Defects. J Cutan Aesthet Surg. 2023 Jul-Sep;16(3):245-251. doi: 10.4103/JCAS.JCAS_168_22. PMID: 38189074; PMCID: PMC10768961.
- McGregor John C, A clinical assessment of the bilobed flap. PII: S0007-1226(81)80094-X
- Esser J. Gestielte locale Nasenplastik mit zweizipfligem Lappen, Deckung des se-kundaren Defktes vom ersten Zipfel durch den Zweiten. Dtsch Z Chir 1918;385–90.