Cases
Browse peer-reviewed surgical case reports.

Case 20 2026: Staged Excision and Delayed Primary Closure of a large Nodular Basal Cell Carcinoma of the Anterior Scalp
Mikkel Halborg Sørensen, Nanja Gotland Sundstrup, Christian Lyngsaa Lang
Keywords: Basal cell carcinoma, scalp reconstruction, staged excision, primary closure, scalp biomechanics. Authors: Mikkel Halborg Sørensen, MD; Nanja Gotland Sundstrup, MD; Christian Lyngsaa Lang, MD. Institution: Department of Plastic Surgery and Burns, Rigshospitalet, Copenhagen University Hos-pital, Denmark Abstract A 48-year-old woman was referred with a non-radically excised nodular basal cell carcinoma of the anterior scalp complicated by wound infection and dehiscence. Re-excision with 3 mm margins to the galea was performed under local anesthesia. Given local inflammation and uncertain margin status, delayed reconstruction was planned pending histopathological confirmation. After clear margins were verified, controlled subgaleal undermining allowed tension-reduced primary closure. This staged strategy ensured oncologic safety while preserving hair-bearing scalp and avoiding unnecessary flap reconstruction. Patient medical history A 48-year-old woman was referred after incomplete excision of a nodular basal cell carcinoma (nBCC) of the anterior scalp performed in private plastic surgery practice. Histology demonstrated tumor involvement of the lateral margins, while the deep margin was free of tumor. Postoperatively, wound rupture and infection developed. Microbiology showed sparse growth of Staphylococcus aureus, and antibiotic therapy was initiated. The patient was otherwise non-smoking and healthy, with well-treated asthma, as her only relevant comorbidity. Before and After Patient examination Clinical examination revealed a 22 × 19 mm anterior scalp defect with limited perifocal erythema and minimal purulent discharge. No regional lymphadenopathy was palpable. Pre-operative considerations Initial histopathology demonstrated nodular basal cell carcinoma with focal lateral margin involvement and a clear deep margin, without perineural invasion or other high-risk features. In accordance with current recommendations for low-risk BCC, re-excision with 3 mm c

Case 22 2026: Superior Gluteal vessel: A rarely used recipient for free flap reconstruction of lumbosacral defects: a case report.
Tushar Dutta, Arun PS, Swati Sattavan
Keywords: Superior gluteal vessel, free flap reconstruction, lumbosacral defects Authors: 1. Tushar Dutta, Consultant Plastic Surgeon; 2. Arun PS, Consultant Surgical Oncologist; 3. Swati Sattavan, Consultant Surgical Oncologist; Institute: State Cancer Institute, Guwahati, Assam, India Abstract Lumbosacral defects that are too large for local flap reconstruction should be considered for microvascular free tissue transfer. However, lack of suitable recipient vessels in the area makes the task technically difficult. Options such as thoracodorsal and inferior gluteal vessels extended with vein grafts and AV loops have been described. Each option has its own drawbacks. Despite having a short course at its origin, the superior gluteal vessel is a viable alternative. We describe here a case where the vessel was dissected out with adequate length and used as a recipient for free flap reconstruction. Patient medical history The patient was a 41-year-old lady with no known comorbidities. She presented to us with a large lumbosacral mass that had been growing for one year. Before visiting our center, she had been operated twice at other institutions and had recurrences after each occasion. During the last three months the mass had started to grow rapidly and caused ulceration. There was no pain or fever. There was no neurological involvement of lower limbs. Patient had an ECOG status 1. Before and After Patient examination A 17x 22 cm mass was noted encompassing the left part of lumbosacral region and crossing the midline to the opposite side. The superior limit of the lesion was at the L3 vertebra and inferior extent was near the coccyx. Skin ulceration was noted at the center of the mass. On palpation, the mass was warm to touch, hard in consistency and immobile. Skin was fixed and fixity was also noted to the underlying muscle. No tenderness was elicited. Surrounding possible donor sites for flap harvest showed no scars. Pre-operative considerations Preoperative biopsy co

Case 23 2026: “Minimally Invasive Finger Amputation Using a Volar ‘Toilet seat’ Flap for Invasive Squamous Cell Carcinoma”
Claes Hannibal Killerich, Nikolaj Warming
Keywords: Squamous cell carcinoma; finger amputation; volar flap; local reconstruction; traction neurectomy; hand surgery. Authors: Claes Hannibal Killerich, Nikolaj Warming Abstract A 93-year-old woman presented with a chronic non-healing dorsal finger wound initially diagnosed as actinic keratosis. Repeat biopsy revealed invasive squamous cell carcinoma with joint and bone involvement. Due to the extent of invasion, distal amputation of the third finger was required. Reconstruction was performed using a volar “toilet seat” flap under digital nerve block to minimize surgical burden. The procedure achieved clear margins, preserved stump length, and avoided donor-site morbidity. This case highlights the importance of early re-biopsy of non-healing lesions and adapting surgical strategy to patient age, function, and comorbidity. Patient medical history A 93-year-old woman presented with a wound on the dorsal aspect of the proximal phalanx of the left third finger. A primary biopsy revealed actinic keratosis, and the lesion was treated several times with curettage and electrodesiccation by a private dermatologist. Despite repeated treatments under professional supervision, the wound failed to heal.Due to the persistent non-healing nature of the lesion, a repeat biopsy was performed, confirming the diagnosis of squamous cell carcinoma (SCC). The patient was referred to the Department of Plastic Surgery, Aalborg University Hospital, where a primary excision was performed with a 7 mm surgical margin. Histopathological examination demonstrated invasive tumor growth involving both joint and bone. The defect was subsequently reconstructed using a full-thickness skin graft. Before and After Patient examination The left third finger showed a healed full-thickness skin graft on the dorsal aspect of the proximal phalanx, covering the proximal interphalangeal (PIP) joint. There was no visible residual tumor, and no palpable lymphadenopathy in the left cubital fossa or axillary re

Case 25 2026: Closed Reduction of a Distal Radius Fracture in the Emergency Department
Maria Lerche Mortensen and Philip Månsson
Keywords: Distal radius fracture, closed reduction, fracture management, Colles’ fracture, orthopedic injury Authors: Maria Lerche Mortensen and Philip Månsson. Institution: Department of Orthopedic Surgery, SUH Nykøbing Falster, Denmark Abstract A 62-year-old female presented to the emergency department after a fall from standing position, attempting to break the fall with her left hand. She presented with pain, swelling, and a visible deformity of the wrist. A distal radius fracture of Colles’ type was diagnosed. She was treated in the emergency department in accordance with local guidelines, with closed reduction using both Chinese finger traps and manual reduction with a hematoma block for analgesia. Finally, a dorsal below-elbow cast was applied, and the patient was referred for follow-up after 10-12 days. Patient medical history This patient was active and employed, able to take care of herself, her family and household. She had no past fractures, no relevant medication, and no known allergies. Before and After Patient examination Patient history was obtained, involving circumstances of the trauma, including reasons to suspect underlying disease or other injuries. She fell while walking on a slippery surface, described the trauma as “just bad luck”, she reported no other complaints of pain, had intact memory, and had no cardiac symptoms prior to fall. The clinical examination included inspection, palpation, and function. Inspection: A bayonet deformity was observed, with significant swelling over the radial styloid. There were no wounds or discoloration. Palpation: There was a palpable step-off, and pain over the distal radius. Elbow, hand and fingers were palpated without pain. Therefore, there was no suspicion of other injuries. Function: Neurological and vascular integrity were intact. The motor function was tested: n. ulnaris – finger abduction with intact strength; n. radialis – extension of the MCP-joints; n. medianus – opposition of the first digit. The

Case 14 2026: Nail removal and punch biopsy - Subungual Melanoma
Linnea Kristensen Ejiofor
Keywords: Nail removal, nail bed biopsy, nail punch biopsy, Subungual Melanoma Authors: Linnea Kristensen Ejiofor, MD, Department of Plastic Surgery and Burns Treatment, Copenhagen University Hospital, Rigshospitalet, and Magnus Balslev Avnstorp, Specialist plastic surgeon, Zealand University Hospital, Roskilde. Abstract Nail changes can reflect a wide spectrum of benign and malignant conditions, making accurate clinical evaluation essential. This case report reviews key background knowledge on common nail alterations and their differential diagnoses. It aims to support clinicians in recognizing when a nail biopsy is indicated and outlines practical considerations for performing the procedure. In addition, the report describes essential steps in the biopsy technique and provides guidance on appropriate postoperative management and follow-up. Patient medical history A 72-year-old man was referred to the department of plastic surgery and breast surgery at Zealands University Hospital, Roskilde, on suspicion of malignant melanoma under the nail of his right thumb. Before and After Patient examination The patient presented with hutchinson’s sign, longitudinal melanonychia and no swollen lymphnodes. He had no first-degree relatives with melanoma, no prior history of melanoma (invasive or in situ) and no prior history of other skin cancers. Pre-operative considerations Background on Subungual Melanoma (SM) SM is a rare but serious malignancy arising from the nail matrix. Early diagnosis is crucial for treatment and prognosis. Nail changes are often benign; however, malignancy must always be considered in cases of pigmented nail lesions, particularly longitudinal brown or black streaks (longitudinal melanonychia). Biopsy is required when diagnostic uncertainty persists after clinical and dermoscopic evaluation. The incidence of SM is not directly associated with ethnicity in terms of increased risk; however, SM accounts for up to 33% of all melanoma cases in individuals wi
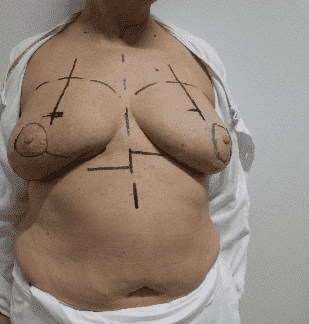
Case 15 2026: The Goldilocks mastectomy
Nanja Gotland Sundstrup (MD), Pia Cajsa Leth Andersen (MD)
Keywords: Goldilock, Mastectomy, Goldilocks mastectomy, Breast reconstruction, mamma reconstruction, Oncoplastic, Risk reducing mastectomy, breast cancer, cancer Authors: Nanja Gotland Sundstrup (MD), Pia Cajsa Leth Andersen (MD) Institution: Department of Plastic Surgery and Burns, Rigshospitalet, Copenhagen University Hospital, Denmark Abstract This case report describes the “Goldilocks procedure” as a technique used for primary breast reconstruction in a patient with prior bilateral c. mamma, treated with lumpectomy and radiotherapy. An implant-based reconstruction was not advised due to the radiotherapy, and she was reluctant to undergo larger scale autologous reconstruction. She was suggested the “goldielocks procedure” as an upgrade to the simple mastectomy which was her alternative consideration. the Goldilocks procedure has the advantage of achieving immediate formation of a small breast, while simultaneously establishing a favorable platform for potential delayed reconstruction with autologous fat grafting. Patient medical history The patient, a 67-year-old woman had a history of bilateral breast cancer: left-sided in 2016 and right-sided in 2023, treated with lumpectomy, and radiotherapy, with additional chemotherapy for the right-sided cancer. Further she was found to carry a pathogenic CHEK2 mutation. The patient underwent bilateral risk reducing mastectomy using the Goldilocks technique, with maximal preservation of the skin envelope and subcutaneous tissue (1). Compared with a simple mastectomy, this approach preserved a good shape and projection resulting in the formation of a small breast. Furthermore, the result provided a more favorable foundation for potential delayed breast reconstruction. The patient was planned for a reconstruction in terms of lipofilling, and mastopexy as well as nipple reconstruction. Before and After Patient examination The patient generally presented with good skin quality. Clinical examination revealed sequelae of prior br

Case 17 2026: Papilla Reconstruction Using the Tennessee Flap Following DIEP Flap Breast Reconstruction
Mikkel Halborg Sørensen, Nanja Gotland Sundstrup, Christian Lyngsaa Lang
Keywords: Tennessee flap, modified C-H flap, nipple reconstruction, invasive ductal carcinoma, DIEP flap, secondary breast reconstruction Authors: Mikkel Halborg Sørensen, MD; Nanja Gotland Sundstrup, MD; Christian Lyngsaa Lang, MD Institution: Department of Plastic Surgery and Burns, Rigshospitalet, Copenhagen University Hospital, Denmark Abstract A 50-year-old woman with a history of invasive ductal carcinoma (IDC) underwent right-sided papilla reconstruction following secondary deep inferior epigastric perforator (DIEP) flap breast reconstruction. A Tennessee flap technique was used in conjunction with correction of lateral volume of the DIEP flap. The technique provided projection and predictable positioning relative to the contralateral nipple-areola complex. The procedure was performed under local anesthesia in an outpatient setting. The immediate postoperative appearance was satisfactory, and wound healing proceeded without complications. This case higlights the continued utility of the Tennessee flap as a simple, safe, and reproducible technique for delayed nipple reconstruction. Patient medical history A 50-year-old woman with a history of IDC underwent right-sided subcutaneous mastectomy in 2017. In 2025, she underwent unilateral delayed autologous breast reconstruction using a DIEP flap. In 2026, completion of the reconstructive process was planned with papilla reconstruction. The patient was in good general health, non-smoking, and without known comorbidities. Before and After Patient examination Clinical examination demonstrated a well-integrated right-sided DIEP flap, good symmetry compared to the contralateral breast, even though the flap was too voluminous at the lateral side. Absence of nipple-areola complex (NAC) on the reconstructed side and a contralateral areola with soft and not sharply demarcated borders. A well-healed lower abdominal donor-site scar from the DIEP flap harvest was present. Pre-operative considerations In Denmark, the Tennessee

Case 18 2026: Nipple reconstruction on a DIEP-flap after breast cancer
Alaa Jady, Pia Cajsa Leth Andersen
Keywords: Nipple reconstruction, plastic surgery, DIEP flap, C-V flap, Tennessee flap Authors: Alaa Jady, MD, Pia Cajsa Leth Andersen, MD. Copenhagen University Hospital, Rigshospitalet. Denmark. Abstract Nipple reconstruction is an important final step in breast reconstruction after mastectomy. This case describes a 42-year-old woman with prior right-sided breast cancer who underwent successful breast reconstruction using a DIEP flap followed by nipple reconstruction with the Tennessee technique. Pre-operative planning focused on achieving symmetry through detailed bilateral measurements and nipple–areola sizing. The procedure involved designing a flap with two arms and a rounded head, careful preservation of the subdermal plexus, and staged suturing. Postoperative follow-up showed good healing, maintained nipple projection, and satisfactory symmetry three months after surgery. Patient medical history A 42-year-old woman with a known history of Hashimoto’s thyroiditis was diagnosed with right-sided breast cancer in June 2022. She received neoadjuvant therapy followed by a right-sided mastectomy in December 2022 and adjuvant radiotherapy. Following completion of these treatments, the patient was deemed cancer-free. In November 2024, she underwent uncomplicated right-sided breast reconstruction using a deep inferior epigastric perforator (DIEP) flap and a contralateral mastopexy for symmetry. Subsequently, right-sided nipple reconstruction was performed in December 2025. Before and After Patient examination Physical examination revealed well-healed scars on both breasts that appeared soft and symmetrical. At the site of the DIEP flap on the right breast, the nipple was absent. Pre-operative considerations Since the patient planned to undergo subsequent nipple–areola complex (NAC) tattooing following our reconstruction, a nipple reconstruction using the “Tennessee” technique was chosen. To achieve symmetry, bilateral measurements were obtained with the patient in the

Case 26 2026: Dual-Hybrid Flap Advancement for Proximal Dorsal Nasal Reconstruction
Lukas Kure-Rosenberg, Magnus Balslev Avnstorp
Keywords: SCC, Flap, Reconstruction, Nose, Novel, Hybrid Authors: Lukas Kure-Rosenberg, Magnus Balslev Avnstorp , Department of Plastic- & Breast Surgery, Zealand University Hospital, Denmark. Abstract Background: Proximal dorsal nasal defects are commonly reconstructed with glabellar advancement flaps. However, in selected patients with favorable distal tissue mobility, alternative local strategies may provide equivalent reconstruction while preserving aesthetic subunits thus minimizing scar burden. Case Presentation: An 84-year-old male underwent oncologic excision of a 13-mm moderately differentiated squamous cell carcinoma of the proximal nasal dorsum. The resulting full-thickness defect extended toward the nasal bulb. Preoperative assessment showed significant bulbous skin mobility and distal redundancy without prior surgical scarring. Methods: Instead of glabellar recruitment, reconstruction was performed with a hybrid local advancement strategy combining Peng-inspired medialization with a limited Rintala/H-type advancement component. Tissue was mobilized in the subcutaneous plane to preserve the subdermal plexus, and distal advancement was maintained lateral to the midline to protect dorsal contour symmetry. Results: Flap perfusion remained stable, with no ischemia or venous congestion. At the two-month follow-up, the patient showed a preserved dorsal contour, symmetrical nasal lines, and satisfactory scar placement, without trapdoor deformity or tip distortion. Conclusion: Selected proximal dorsal nasal defects can be reconstructed with hybrid local advancement techniques that strategically exploit distal tissue redundancy. Context-driven modification of established flap principles may allow avoidance of glabellar flaps while maintaining excellent functional and aesthetic outcomes. Patient medical history An 84-year-old male was referred to the Department of Plastic Surgery at Roskilde Sealand University Hospital, Denmark, in winter 2025 by a dermatologi

Case 02 2026: Tarsoconjuctival Flap for Eyelid Reconstruction
Ajla Sabitovic, Rikke Børthy Petersen, Nanja Gotland Sundstrup
Keywords: Basal Cell Carcinoma, Skin Cancer, Eyelid Reconstruction, Tarsoconjuctival flap. Authors: Ajla Sabitovic, MD, Rikke Børthy Petersen, MD, Nanja Gotland Sundstrup, MD. Abstract This case describes the use of a tarsoconjuctival flap for reconstruction of the lower eyelid following excision of a basal cell carcinoma in a 76-year-old woman. Due to the tumor size, depth and location near the limbus of the eye, direct closure was not possible. The tarsoconjuctival flap was chosen as the preferred reconstructive approach because of its ability to reconstruct all layers of the eyelid. Postoperative follow-up at six months demonstrated satisfactory aesthetic and functional outcomes. Patient medical history A 76-year-old woman presented with a biopsy-confirmed nodular basal cell carcinoma involving the right lower eyelid. Tumor excision was performed in general anesthesia with 3 mm margin and intraoperative frozen-section control, confirming tumor free margins. Resection resulted in a full-thickness defect involving approximately 90% of the lower eyelid. Reconstruction was performed with a tarsoconjuctival flap for the posterior lamella and a Tripier flap from the upper eyelid for the anterior lamella. Before and After Patient examination Clinical examination revealed a 12 x 10 mm elevated ulcerating lesion involving the right lower eyelid, extending into conjunctiva and limbus. Pre-operative considerations The patient presented with a full-thickness defect of the lower eyelid involving conjunctiva and the inferior eyelid margin. Due to the tumor size and location direct closure was not possible. Reconstruction with a flap was therefore required to secure reconstruction of all layers of the lower eyelid to give the eyelid full support and thereby secure its function. 1 Step 1 Preoperative skin markings outlining the tumor and 3 mm excision margin. 2 Step 2 Excision of the tumor was performed with a 3 mm margin, involving the conjunctiva, tarsal plate and lower eyelid

Case 04 2026: Full-Thickness Skin Graft for Areola Reconstruction: A Simple and Reliable Technique
Ajla Sabitovic (MD), Nanja Gotland Sundstrup (MD)
Keywords: Breast cancer, Areola reconstruction, Full-Thickness Skin Graft. Authors: Ajla Sabitovic (MD), Nanja Gotland Sundstrup (MD) Abstract This case describes the use of full-thickness skin graft for reconstruction of areola in a 64-year-old woman following right-sided mastectomy and delayed breast reconstruction with a DIEP flap. The patient preferred autologous reconstruction and declined tattooing or additional donor-site scars. Due to the light pigmentation on the contralateral areola, it was decided to shave the skin off as a full-thickness in the affected area, and let the following scaring in the area lead to a little change in pigmentation and contration. This approach avoided additional scarring while achieving an acceptable aesthetic result. Patient medical history A 64-year-old woman with a history of right-sided breast cancer underwent mastectomy in November 2022. In August 2024, the patient received a breast reconstruction with a free DIEP flap and a contralateral breast reduction. Nipple reconstruction using af full-thickness skin graft was subsequently performed in March 2025. In October 2025, the patient underwent areola reconstruction with a full-thickness skin graft on the reconstructed breast, combining the donor and recipient site around the nipple. Before and After Patient examination Clinical examination revealed aesthetically pleasing results following the DIEP flap and papil reconstruction as well as a light-colored contralateral areola. Pre-operative considerations It was considered to use a skin-graft from the groin due to its darker pigmentation, but the patient didn’t want any additional scares. Due to the light pigmentation on the contralateral areola, a local full-thickness skin graft was harvested at the recipient site. Postoperative scarring was expected to provide mild pigmentation change and contraction to improve areola definition. 1 Step 1 Preoperative markings performed with the patient in a standing position, showing the neo

Case 06 2026: Post-Embolic Gangrene of the Left Lower Limb Managed with Serial Debridement, VAC Therapy, and Cross-Leg Free Flap Reconstruction for Limb Salvage
Dr. RAHUL KAPOOR
Keywords: Rheumatic Heart Disease, Embolism, Gangrene, Limb Salvage, Vessel-Depleted Extremity, Cross Leg Free Flap Authors: DR RAHUL KAPOOR Abstract Limb salvage in a vessel-depleted extremity remains a formidable reconstructive challenge. We report a case of extensive lower limb gangrene following popliteal artery embolism in a patient with rheumatic heart disease and mitral stenosis. The defect involved exposed bone, necrotic tendons, and absent distal perfusion, with ipsilateral recipient vessels unsuitable for microvascular anastomosis. A cross-leg free flap with external fixation was performed using contralateral posterior tibial vessels. Venous congestion required supercharging with great saphenous vein anastomosis. The postoperative course was uneventful. Flap division at eight weeks demonstrated successful neovascularization, achieving durable limb salvage with progressive sensory and perfusion recovery at 18 months follow-up. Patient medical history Known case of Rheumatic Heart Disease with Mitral Stenosis. Patient developed complain of pain in left leg and foot, in June, 2024. Peripheral Angiography showed 80-90% occluded left external iliac artery & left popliteal artery and 100% left posterior tibial artery. Thrombolysis and plain old balloon Angioplasty done after 3 days of development of pain. Revascularization procedure was followed by development of compartment syndrome in left leg and foot and fever, with progressive discoloration of skin over lower half of leg, ankle and dorsum of foot. Discolouration turned into open wound with complete loss of skin cover, necrosed tendons and exposed bones of lower half of leg, ankle joint and proximal half of dorsum of foot. wound was heavily infected with pus discharge and foul smell. Before and After Patient examination there was progressive discoloration of skin over lower half of leg, ankle and dorsum of foot. Discoloration turned into open wound with complete loss of skin cover, necrosed tendons and e

Case 07 2026: Reconstruction of a Complex Epigastric Abdominal Wall Defect Following Wide Excision of Giant Fibrosarcoma Using Prolene mesh and Modified Keystone Flap in a Resource-Limited Setting: A Case Report”
Abdirahman Abdifatah Mohamed, Numan Omar Ibrahim, Rose Alenyo, Kalanzi Edris
Keywords: fibrosarcoma; Soft tissue sarcoma; Abdominal wall tumor; Wide local excision; Keystone flap; Uganda Authors: Abdirahman Abdifatah Mohamed, MD Final Year PRS Trainee 1, Numan Omar Ibrahim, MD PRS Trainee 2, Rose Alenyo, MD Consultant Plastic Surgeon 3, Kalanzi Edris, MD Senior Consultant Plastic Surgeon 4. Abstract Fibrosarcoma is a rare soft tissue sarcoma with aggressive local infiltration and high recurrence risk. We present a 71-year-old Ugandan man with a giant epigastric fibrosarcoma causing a complex abdominal wall defect. Imaging showed invasion of subcutaneous tissue and rectus muscle without metastasis. The patient underwent wide local excision with 5 cm margins, followed by reconstruction using Prolene mesh and a modified keystone flap with skin grafting. Recovery was uneventful, demonstrating effective surgical and reconstructive management in a resource-limited setting. Patient medical history a 71-year-old male who presented with a two-year history of a progressively enlarging anterior abdominal wall mass. The lesion initially appeared as a small, firm nodule and gradually increased in size, eventually becoming a large, fungating tumor associated with ulceration, necrosis, and intermittent bleeding. There was no history of distant symptoms suggestive of metastasis. Imaging confirmed a locally invasive epigastric mass involving the subcutaneous tissue and rectus abdominis muscle, without visceral or distant spread. Before and After Patient examination On physical examination, the patient had a large, exophytic, fungating mass located in the supraumbilical (epigastric) region of the anterior abdominal wall. The lesion was deeply invasive with irregular margins and was associated with ulceration, areas of necrosis, and active bleeding. The overlying skin was stretched, tense, and partially ulcerated. The mass appeared fixed to the underlying abdominal wall musculature, suggesting muscle involvement. There were no clinical signs of peritoneal invo

Case 09 2026: Single-Stage Spear Flap Reconstruction of Recurrent Full-Thickness Nasal Alar Defects: A Two-Case Series
Lukas Kure-Rosenberg, Matilda Svenning, Mille Vissing. Magnus Balslev Avnstorp
Keywords: Spear flap; nasolabial turnover flap; nasal ala reconstruction; basal cell carcinoma; case series Authors: Lukas Kure-Rosenberg, Matilda Svenning, Mille Vissing. Magnus Balslev Avnstorp Abstract Background: Reconstructing the full thickness of the nasal ala is technically challenging because it requires restoring contour, lining, and airway patency all at once. The Spear flap, also known as the nasolabial turnover flap, remains a useful single-stage option for selected lateral alar defects. Cases: Two elderly women presented with recurrent basal cell carcinoma of the ala nasi following multiple prior curettages. In case 1, excision resulted in a 20 × 12 mm through-and-through alar defect. In case 2, a recurrent lesion on the left alar measuring 11 × 8 mm initially required staged margin control before final reconstruction. Technique: Both defects were reconstructed using a cheek-based Spear flap after frozen-section-guided excision. Flap design was customized to recreate internal lining and external coverage while minimizing distortion of the alar rim and vestibule. Results: Both flaps remained viable, with no evidence of ischemia or venous congestion. Case 1 achieved complete oncologic clearance and healed with a stable contour; mild residual vestibular fullness did not warrant revision. In case 2, staged clearance allowed for delayed single stage inset, and early healing proceeded without complications. Conclusion: For recurrent through-and-through alar defects, the Spear flap is a reliable and practical reconstructive option. Especially in elderly patients with comorbidities or competing health issues, it provides dependable vascularity, good tissue match, and restores the alar subunit without the complexity of multi-stage procedures. Patient medical history Case 1 (left image) A 90-year-old woman was referred for recurrent basal cell carcinoma of the ala nasi after multiple previous curettages performed in a private dermatology practice in october 2025

Case 01 2026: Secondary Nasal Sidewall Reconstruction After Prior Bilobed Flap Surgery Using a Surrounding Lateral-Based Trilobed Flap
Frederik Penzien Wainer Mamsen & Lukas Kure-Rosenberg
Keywords: Nasal reconstruction following NMSC, Transposition flaps, Utilizing existing flap as design solution Authors: Frederik Penzien Wainer Mamsen & Lukas Kure-Rosenberg Abstract Background: Secondary nasal reconstruction adjacent to prior local flaps poses unique challenges due to scarring, altered tissue mobility, and potentially unpredictable vascular territories. Although bilobed flaps are considered workhorse techniques in nasal reconstruction, their presence may limit options in recurrent malignancy. Strategic flap planning that respects vascular integrity and aesthetic subunits is therefore essential. Case Presentation: A 74-year-old male patient presented with biopsy-proven recurrent basal cell carcinoma of the right nasal sidewall within a previously reconstructed area using a 180-degree bilobed flap. Tumor excision created an 8 × 11 mm defect abutting the prior reconstruction. Direct closure, secondary intention healing, and skin grafting were deemed unsuitable because of the risk of nasal distortion and alar contracture. Methods: A lateral-based trilobed transposition flap was designed to encircle the prior bilobed flap while preserving its vascular pedicle and redirecting perfusion toward unscarred tissue. The first lobe closed the primary defect, and subsequent lobes redistributed tension vectors. Subcutaneous undermining was performed to preserve the subdermal plexus. Results: The flap demonstrated stable perfusion without ischemia or venous congestion. Healing was uneventful. At 1.5-month follow-up, the patient showed great contour with slight pincushion, preserved nasal symmetry, and a favorable color match. Conclusion: In nasal reconstruction adjacent to prior flap surgery, a lateral-based trilobed flap is a safe and effective single-stage option. Careful vascular planning and tension redistribution enable reliable secondary reconstruction with excellent functional and aesthetic outcomes. Patient medical history Introduction Bilobed flap des

Case 05 2026: Partial avulsion of the nasal tip
Nicolai Lassen Frid, Johan Hindkjær Therchilsen, Jakob Gerlach Christensen
Keywords: Trauma, Nasal tip, Avulsion, rhinoplasty Authors: Nicolai Lassen Frid, MD, Johan Hindkjær Therchilsen, MD, Jakob Gerlach Christensen, MD Institution: Department of Otorhinolaryngology and Maxillofacial Surgery, Zealand University Hospital, Køge, Denmark Abstract Traumatic partial avulsion of the nasal tip is a rare condition that can present both functional and aesthetic challenges. This case reports a 58-year-old woman with a partial nasal tip avulsion after a fall onto a metal crate. Examination revealed injury to the lower lateral cartilages with loose cartilaginous fragments. Surgical repair focused on restoration of the structural tip support, using end-to-end sutures for approximation of the cartilage and interdomal suturing. This case focuses on rhinoplasty-based principles in acute management of nasal trauma to preserve projection, symmetry, and long-term stability of the nose. Patient medical history A 58-year-old woman presented to the emergency department with a traumatic partial avulsion of the nasal tip sustained after slipping on ice and striking her face against a metal crate. The patient reported neck soreness but exhibited no signs of concussion and no other facial injuries or neck injuries. She had no prior history of nasal trauma. Her medical history included well-controlled hypertension and chronic back pain. Before and After Patient examination Examination of the external nose revealed a large laceration involving the nasal tip, with partial avulsion on the right side. The lower lateral cartilages were injured, with transection of the right lateral crus, a loose fragment of the right intermediate crus, and bilateral fractures of the medial crura with loose cartilaginous fragments. The skin was intact over the columellar and the left alar surface. The wound edges were well defined and with no tissue loss. Sensation was absent in the lacerated tip, but with preserved capillary refill. Anterior rhinoscopy showed a midline septum without h

Case 24 2026: Ipsilateral Myocutaneous Latissimus Dorsi Flap for Traumatic Upper Limb Soft Tissue and Vascular Injury Following Road Traffic Accident
Sumaira Sattar
Keywords: Latissimus dorsi flap, upper limb trauma, soft tissue reconstruction, vascular injury, degloving injury Authors: Sumaira Sattar, FCPS (Plastic Surgery), Institution: SMBB Institute of Trauma, Karachi, Pakistan Abstract A 20-year-old female presented with a severe traumatic injury to the right upper limb following a road traffic accident involving a pedestrian–motorbike collision with subsequent run-over injury. The trauma resulted in extensive soft tissue loss, degloving injury, and associated vascular compromise. Initial management followed advanced trauma protocols, after which the patient was referred for vascular and reconstructive assessment. Imaging revealed brachial artery thrombosis with segmental radial artery injury; however, hand perfusion was maintained through collateral circulation. Following stabilization and vascular reconstruction using a reverse great saphenous vein graft, soft tissue coverage was achieved with an ipsilateral myocutaneous latissimus dorsi flapThe flap provided durable coverage of exposed vital structures and the elbow joint without the need for microsurgical anastomosis. At three-month follow-up, the patient demonstrated excellent functional recovery with satisfactory aesthetic outcome. This case highlights the reliability of the latissimus dorsi flap in complex traumatic upper limb reconstruction. Patient medical history A 20-year-old unmarried female, with no known comorbidities, presented to the emergency department five hours after a road traffic accident involving a bike-versus-pedestrian collision. Following the initial fall, the patient sustained a secondary run-over injury to the right upper limb. There was no history of loss of consciousness, head injury, or trauma to other body regions. Initial assessment and stabilization were performed according to trauma protocols, following which the patient was referred to the plastic and vascular surgery teams for definitive management of the limb injury. Before and After

Case 03 2026: Emergency limb salvage with combined free vastus lateralis and anterolateral thigh flap after post-traumatic brachial artery graft thrombosis in a 16-year-old patient
Dr. Ibrahim Güler
Keywords: Limb salvage, free flap, anterolateral thigh flap, vastus lateralis, brachial artery injury, Gustilo–Anderson IIIC, microsurgery, trauma reconstruction Authors: Dr. Ibrahim Güler, Prof. Dr. Cenk Demirdöver . Department of Plastic, Reconstructive and Aesthetic Surgery, Dokuz Eylül University, Izmir, Turkey; Department of Plastic, Aesthetic and Hand Surgery, Otto von Guericke University, Magdeburg, Germany Abstract A 16-year-old female sustained a crush injury of the left upper extremity, resulting in an open humeral fracture (Gustilo–Anderson IIIC), brachial artery injury, and extensive soft-tissue loss. Initial treatment by trauma and vascular surgery included external fixation and brachial artery reconstruction using a saphenous vein graft. Early graft thrombosis led to critical limb ischemia, and above-elbow amputation was proposed. An emergency limb salvage attempt was performed using a combined free vastus lateralis and anterolateral thigh flap. The limb was successfully salvaged, with a favorable contour and good long-term functional outcome after secondary debulking procedures. Patient medical history A 16-year-old previously healthy female sustained a crush injury to the left upper extremity, resulting in an open humeral fracture (Gustilo–Anderson IIIC), brachial artery injury, and extensive soft-tissue loss [1,2]. Initial management by the trauma and vascular surgery teams at the same hospital included external fixation to stabilize the humeral fracture and reconstruction of the brachial artery using a saphenous vein interposition graft. Early thrombosis of the vein graft led to critical limb ischemia, and above-elbow amputation was subsequently proposed. Before and After Patient examination On examination by the plastic surgery team, the left upper extremity showed extensive soft-tissue loss around the elbow and proximal forearm, with the humerus stabilized in an external fixator. Despite the thrombosis of the brachial artery interposition graft,

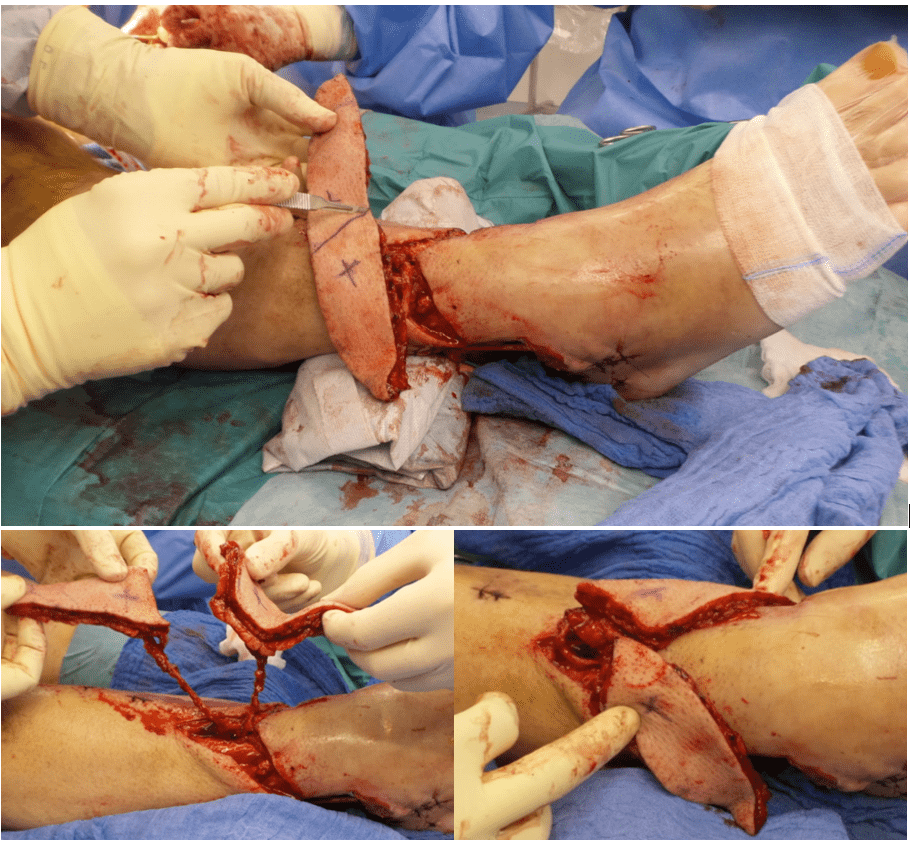
Case 16 2026: Severe Foot Degloving Injury Following a Forklift Crush: A Limb-Salvage Case
Cecilie Jansen, Emil Villiam Holm-Rasmussen, Mette Stueland Wolthers. Copenhagen
Keywords: Degloving injury, (decollement), foot trauma, limb salvage, fluorescence angiography, negative pressure wound therapy. Authors: Cecilie Jansen, Emil Villiam Holm-Rasmussen, Mette Stueland Wolthers. Copenhagen University Hospital, Rigshospitalet, Denmark. Abstract A 30-year-old previously healthy man was admitted to The Trauma Centre at Copenhagen University Hospital, Rigshospitalet after his left foot was crushed by a 1.5-ton forklift at work. He sustained a large open fracture and an extensive circumferential degloving injury involving the foot and ankle, while distal perfusion remained intact. Computed Tomography (CT) demonstrated multiple intra-articular fractures with suspected Lisfranc injury and no vascular injury on CT angiography. Following orthopedic stabilization, plastic surgical management focused on debridement, tissue viability assessment, skin and heel-pad preservation, and limb salvage. This case highlights the challenges of severe foot degloving and multidisciplinary limb-salvage management. Patient medical history The patient was previously healthy, had no significant past medical history, and was a non-smoker. Before and After Patient examination On arrival at The Trauma Centre at Copenhagen University Hospital, Rigshospitalet, the patient was hemodynamically stable but slightly pale. He reported paresthesia in the left foot, but gross sensation was preserved. Clinical examination revealed an approximately 15 cm open wound laterally on the left foot with exposed bone and tendon. A palpable pulse was present in the dorsalis pedis artery, whereas the posterior tibial artery pulse was not palpable. Capillary refill and sensation were preserved. A trauma CT scan with intravenous contrast, including CT angiography of the lower leg was performed. Imaging demonstrated multiple intra-articular fractures distal to the talus with widening between the second metatarsal and medial cuneiform, raising suspicion of a Lisfranc injury. Air was present in

Case 12 2026: Closure of defect on ala nasi with modified shark island flap
Mickie Bang Christensen (MD), Magnus Avnstorp (MD)
Keywords: Shark island flap, facial skin defect, BCC, nasal skin cancer, nasal reconstruction, reconstructive surgery Authors: Mickie Bang Christensen (MD), Magnus Avnstorp (MD), Department of Plastic- & Breast Surgery, Zealand University Hospital Roskilde, Denmark Abstract This case presents the use of a modified shark island flap for reconstruction of a defect on the ala nasi following excision of a basal cell carcinoma in a 85-year old male. Due to the tumor size and location, direct closure was not feasible. The shark island flap was chosen as the reconstructive approach. Surgery was done under local anesthesia. Excision of the tumor was done with a 3 mm margin. Histology from frozen sections showed clear margins without malignancy. Postoperative follow up at both one week and two months demonstrated a satisfactory cosmetic outcome and no signs of recurrence. Patient medical history 85-year old male with a medical history of atoxic goiter, hypertension, Parkinson's disease, melanoma and multiple skin carcinomas, was referred with 3 facial skin carcinomas (dorsum nasi, right ala nasi and left side of the upper lip). This case focuses on the carcinoma on the ala nasi. The biopsy showed basal cell carcinoma of nodular subtype. The patient had years prior been operated with a bilobed flap due to a skin carcinoma on the right dorsum nasi, which had resulted in bulging of the right side of the dorsum. Before and After Patient examination Well preserved male with poor skin quality. On clinical examination, a tumor measuring 6 x 5 mm and 2 mm elevation from the surface of the skin was found on the right ala nasi, involving the nasal sulcus. Clinically not adherent to underlying tissue. There were no palpable regional lymph nodes. Pre-operative considerations Surgery and radiation were discussed with the patient. The patient preferred surgery. Due to the tumor size and location, direct closure was not feasible. FTSG would delete the alar-facial sulcus, create a big,

Case 08 2026: A Hella Lamella: A Three-Flap, Full-Thickness Lower Eyelid Reconstruction
Sondre F. Koren (MD), Jette B. Løvenwald (MD). Roskilde, SUH, Denmark
Keywords: Eyelid reconstruction, Hughes flap, tarsoconjunctival flap, periosteal flap, periorbital, scc, cheek rotational flap, Z-plasty Authors: Sondre F. Koren (MD), Jette B. Løvenwald (MD). Roskilde, SUH, Denmark. Abstract An 83-year-old male with atrial fibrillation, stage 4 chronic kidney disease, chronic heart failure, monoclonal gammopathy of undetermined significance (MGUS), and glaucoma presented with a 35 × 35 × 15 mm ulcerated squamous cell carcinoma (SCC) of the lateral right lower eyelid. Frozen section-guided full-thickness excision was performed under general anaesthesia. Reconstruction was accomplished in two stages. In the first stage, a combined pedicled tarsoconjunctival flap and a laterally-based periosteal flap (posterior lamella), and a cheek rotation flap (anterior lamella) were used. Frost sutures provided corneal protection during the 4-week inter-stage interval. In the second stage, flap division was performed under general anaesthesia, incorporating Müller's muscle release to prevent upper eyelid retraction. A small dehiscence at the medial flap junction had resulted in a minor notch, which was ultimately resolved with Z-plasty and release of the underlying inferior scar contracture on the cheek. Final histopathology confirmed highly differentiated SCC with clear margins. The multidisciplinary tumour board found no indication for adjuvant therapy. At 23 days following flap division, the patient was satisfied with the functional and aesthetic result. Patient medical history The patient underwent surgery after a 7-week history of a growing tumour of the cheek and lateral lower eyelid. The punch biopsy reported keratoacanthoma/highly differentiated SCC. The tumour had been observed to assess for spontaneous regression, but continued to grow. He had stage 4 chronic kidney disease, treated with Darbepoetin alfa (Aranesp), and glaucoma treated with Latanoprost eye drops, which he had not been taking for several months, with no documented decline

Case 13 2026: Fillet Flap Reconstruction Following Hemicorporectomy for Recurrent High-Grade Gluteal Sarcoma
Authors: Isha Joshi, Zachary Erlichman, Nia Nikkhahmanesh, Christina Chopra, Jason Ganz
Keywords: Hemicorporectomy, Fillet flap, Spare-parts surgery, Sarcoma reconstruction, Complex pelvic reconstruction Authors: Authors: Isha Joshi MD MBA, Zachary Erlichman MD, Nia Nikkhahmanesh MD, Christina Chopra MD, Jason Ganz MD Institution: Stony Brook University Hospital, Stony Brook, New York Abstract Background: Tissue from non-salvageable limbs may be used in reconstruction of complex defects and represent the principle of the “spare- parts” concept.[1] Fillet flaps advantages include soft tissue coverage of large defects, biocompatibility of an autologous donor, and donor tissue resembling native tissue due to proximity. Case: Fewer than 100 hemicorporectomies have been published in the literature.[2] We present the case of a 53-year-old male who underwent hemicorporectomy for recurrent gluteal sarcoma followed by reconstruction using a near-total thigh fillet flap. Conclusions: Fillet flaps provide soft-tissue coverage of large defects, biocompatible autologous tissue, and donor tissue resembling native anatomy. Patient medical history Primary Diagnosis: In 2015, the patient was diagnosed with a 15-cm high-grade (grade 3) spindle cell carcinoma thought to represent a fibrosarcoma with transformation to dermatofibrosarcoma protuberans, located superior to the buttock. The tumor was resected at an outside hospital (OSH) without perioperative complications. First Recurrence: In 2016, the patient presented to the OSH with recurrent mass in the tumor bed measuring 12.2 cm with erosion of lower coccyx, extension into posterior pelvis, and deviation of the anus. He underwent neoadjuvant radiation and systemic therapy. In 2017, he underwent tumor debulking and permanent diverting colostomy placement. After relocating to New York, he established care at our institution and subsequently underwent conversion of a loop colostomy to an end stoma with mucous fistula in 2020. Secondary Recurrence: In 2022, imaging demonstrated a recurrent tumor above the buttock. The pat

Case 21 2026: Reconstructing the Challenging Eyelid: Hard Palate Graft and Radial Forearm Free Flap Reconstruction in Gorlin–Goltz Syndrome
Miss Ketki Kaushal, Mr Oliver Bassett
Keywords: Gorlin-Goltz Syndrome, Recurrent Basal Cell Carcinoma, Radial Forearm Free Flap, Hard Palate Graft, Oncology, Plastic Surgery, Ophthalmology, Dermatology, Complex Eyelid Reconstruction Authors: Miss Ketki Kaushal, Mr Oliver Bassett Abstract Gorlin-Goltz syndrome, also known as Nevoid Basal Cell Carcinoma Syndrome, is a rare autosomal dominant condition associated with pathogenic variants in the PTCH1 gene and dysregulation of the Hedgehog signaling pathway. A patient with longstanding disease presented with recurrent periocular basal cell carcinoma requiring Mohs excision, resulting in a large full-thickness lower eyelid defect. Reconstruction was performed using a hard palate graft for posterior lamella replacement and a radial forearm free flap with palmaris longus tendon sling for anterior lamella and structural support. Microvascular anastomosis to facial vessels was performed. This case highlights the reconstructive challenges of periocular defects in NBCCS and emphasises multidisciplinary management. Patient medical history A 59-year-old male with a longstanding history of Gorlin–Goltz syndrome (Nevoid Basal Cell Carcinoma Syndrome) diagnosed in 1997 has been under multidisciplinary care involving dermatology, plastic surgery, oncology, and ophthalmology for multiple recurrent basal cell carcinomas. His medical history includes hypertension, iron deficiency anaemia secondary to diverticulosis, chronic gastritis with duodenal ulcer disease, and melanoma in situ of the right knee excised in 2016. He has undergone numerous treatments for cutaneous malignancies including repeated surgical excisions, Mohs micrographic surgery, topical therapies (5-fluorouracil and imiquimod), and reconstructive procedures. In 2012 he underwent Mohs surgery for an infiltrative basal cell carcinoma of the left lower eyelid. Over subsequent years, multiple lesions were treated across the face, temples, ears, forearm, and calf. Since April 2016 he has been managed with the He
Case 19 2026: Split Perforator Flaps for bilateral ankle defects: A modern microsurgical approach to preserve function and reduce secondary thinning operations
Luisa Lotter¹, Marta Jezierska¹, Ilja W. Käch¹, Volker J. Schmidt¹
Keywords: Lower extremity; Orthoplastic Reconstruction; Split flap; microsurgery Authors: Luisa Lotter¹, Marta Jezierska¹, Ilja W. Käch¹, Volker J. Schmidt¹; ¹Department of Plastic Surgery and Handsurgery, HOCH, Health Ostschweiz, Cantonal Hospital St.Gallen, St.Gallen, Switzerland Abstract 46-year-old man presented with two full-thickness soft-tissue defects of the distal right lower leg (medial 7 × 4 cm, lateral 10 × 5 cm) with exposed tendons, osteosynthesis material, and bone after a Gustilo grade IIIb open tibial and fibular fracture. During initial orthopedic stabilization, interdisciplinary orthoplastic assessment and planning were performed. Because of exposed functional structures and two spatially separated defects with healthy anterior skin between them, microsurgical free-tissue reconstruction was chosen to provide stable coverage while preserving the anterior skin and preventing flap-related functional impairment. Reconstruction was achieved using a split anterolateral thigh (ALT) flap based on two independent perforators, enabling simultaneous coverage of both defects with a single vascular pedicle. Patient medical history The patient’s medical history was significant for type 2 diabetes mellitus, two-vessel coronary artery disease, and obesity. Before and After Patient examination Clinical assessment revealed two full-thickness defects at the distal lower leg: • medial defect: 7 × 4 cm with exposed tendons • lateral defect: 10 × 5 cm with exposed bone and osteosynthesis material Both wounds showed non-viable soft-tissue components requiring radical surgical debridement prior to reconstruction. An CT-angiography was performed, revealing a regular three-vessel supply to the affected lower right leg. Preoperative color-duplex-ultrasound was routinely performed to identify the ALT perforator pattern and to verify, if a two-perforator split ALT-fashion is possible. Due to our tertiary orthoplastic program final interdisciplinary reconstruction was schedule
Propeller Flap Based on Two Perforators of the Scapular Artery for the Management of a Severely Traumatized Upper Extremity
Nelson Ramirez Lozano, Alejandro Angelillis Osorio
Oncólogos de Occidente, Manizales, Colombia
Split Perforator Flaps for Bilateral Ankle Defects
Luisa Lotter, Marta Jezierska, Ilja W. Käch, Volker J. Schmidt
HOCH, Cantonal Hospital, St. Gallen, Switzerland
Reconstructing the Challenging Lower Eyelid: Hard Palate Graft and Radial Forearm Free Flap Reconstruction in Gorlin–Goltz Syndrome
Ketki Kaushal, Oliver Bassett
James Cook University Hospital, Middlesbrough, England
Fillet Flap Reconstruction Following Hemicorporectomy for Recurrent High-Grade Gluteal Sarcoma
Isha Joshi, Zachary Erlichman, Nia Nikkhahmanesh, Christina Chopra, Jason Ganz
Stony Brook University Hospital, New York, USA
A Hella Lamella: A Three-Flap, Full-Thickness Lower Eyelid Reconstruction
Sondre F. Koren, Jette B. Løvenwald
Zealand University Hospital, Roskilde, Denmark
Closure of Defect on Ala Nasi with Modified Shark Island Flap
Mickie Bang Christensen, Magnus Avnstorp
Zealand University Hospital, Roskilde, Denmark
Severe Foot Degloving Injury Following a Forklift Crush: A Limb-Salvage Case
Cecilie Jansen, Emil Villiam Holm-Rasmussen, Mette Stueland Wolthers
Rigshospitalet, Copenhagen University Hospital, Denmark
Emergency Limb Salvage with Combined Free Vastus Lateralis and Anterolateral Thigh Flap after Post-Traumatic Brachial Artery Graft Thrombosis in a 16-Year-Old
Ibrahim Güler, Cenk Demirdöver
Dokuz Eylül University, Izmir, Turkey & Otto von Guericke University, Magdeburg, Germany
Ipsilateral Myocutaneous Latissimus Dorsi Flap for Traumatic Upper Limb Soft Tissue and Vascular Injury Following a Road Traffic Accident
Sumaira Sattar
SMBB Institute of Trauma, Karachi, Pakistan

Case 10 2026: Propeller Flap Based on Two Perforators of the Scapular Artery for the Management of a Severely Traumatized Upper Extremity
Nelson Ramirez Lozano. Plastic Surgery, Oncólogos de Occidente Manizales
Keywords: arm, perforator flap, mangled, flap, plastic surgery Authors: Nelson Ramirez Lozano. Plastic Surgery, Oncólogos de Occidente Manizales, Hospital de Santa Sofía Manizales, Colombia. Alejandro Angelillis Osorio. Surgical Assistant, Oncologos de Occidente, Manizales, Colombia. Abstract We present the successful case of a patient who sustained severe trauma to the upper extremity caused by a sugarcane mill (trapiche). We consider this type of trauma to be a reconstructive challenge given the significant degree of soft tissue compromise, the presence of infection in nearly all such cases, and the imperative need for these patients to return to their daily activities. A propeller flap based on two perforators of the scapular artery was designed and executed, enabling adequate reconstruction and wound coverage without generating donor-site morbidity, facilitating early rehabilitation and rapid functional recovery. Patient medical history A male patient sustained severe trauma to the left upper extremity involving a sugarcane mill during occupational activities. He was admitted to the emergency department, where hemostasis was achieved and hemodynamic stabilization was attained. On initial evaluation, no fractures were identified; however, the patient presented with humeral bone exposure, circumferential soft tissue loss involving the upper arm, restricted range of motion, and altered sensation. He subsequently underwent multiple irrigation and debridement procedures, as well as serial negative pressure wound therapy (NPWT) dressing changes performed by the Orthopedics and Traumatology service, achieving adequate control of necrotic tissue and resolution of infection. Plastic Surgery consultation was then requested. Before and After Patient examination The patient presented with a circumferential soft tissue defect of the left upper arm with exposed humerus, no active signs of infection, and an in-situ negative pressure wound therapy device. Physical examination a

Case 11 2026: Dual Internal Mammary Artery Perforator Propeller Flap for Anterior Chest Wall Reconstruction
Nelson Ramirez Lozano. Oncólogos de Occidente Manizales, Alejandro Angelillis Osorio. Surgical Assistant, Oncologos de Occidente, Manizales, Colombia
Keywords: chest wall reconstruction, internal mammary artery, perforator flap, propeller flap, plastic surgery, squamous cell carcinoma, Mohs surgery Authors: Nelson Ramirez Lozano. Oncólogos de Occidente Manizales, Hospital de Santa Sofía Manizales, Colombia Alejandro Angelillis Osorio. Surgical Assistant, Oncologos de Occidente, Manizales, Colombia. Abstract Reconstruction of anterior chest wall defects following skin cancer resection represents a significant surgical challenge. We report a successful case utilizing a propeller flap based on two perforators of the internal mammary artery for reconstruction, achieving stable soft tissue coverage without generating additional donor-site deformity. Patient medical history A male patient in his sixth decade of life was referred with an anterior chest wall defect measuring approximately 8 × 12 cm in diameter, resulting from resection of a squamous cell carcinoma via Mohs micrographic surgery. A propeller flap was designed, two perforators were identified intraoperatively, microsurgical dissection was performed, and flap rotation was executed. Before and After Patient examination Anterior chest wall defect measuring approximately 8 × 12 cm in diameter with imminent risk of osseous exposure. Pre-operative considerations The reconstructive goals were defined as follows: Provision of durable and stable soft tissue coverage Avoidance of additional donor-site morbidity Prevention of secondary deformity at the donor site 1 Flap Dissection The flap design was planned in this configuration for two reasons: 1) alignment with the anatomical axis of the internal mammary artery perforators; and 2) donor site closure oriented to prevent additional contour deformity. 2 Perforator Selection Perforators were selected based on: 1) palpable Doppler-confirmed pulse; and 2) proximity to the pivot point to allow adequate arc of rotation. 3 Isolated Perforators Following meticulous dissection of the selected perforators, complete flap rotati

Case 17: Immediate Proximal Row Carpectomy for combined Scaphoid and Lunate Dislocation Without Fracture
Jorge Jimenez Lopez, Anastasia Boptsi, Konstantinos Kalousis
Keywords: Hand surgery; wrist; carpectomy; scaphoid; lunate dislocation Authors: Jorge Jimenez Lopez, MD; Anastasia Boptsi, MD; Konstantinos Kalousis, MD Institution: Universitätsklinikum Schleswig-Holstein Lübeck Abstract Carpal dislocation fractures are uncommon injuries, most frequently associated with high-energy trauma. Combined carpal dislocations without associated bone fractures are even rarer. Delayed treatment can have serious consequences. The case presented here involves an 86-year-old man with dislocation of the scaphoid and lunate bones, as well as acute carpal tunnel syndrome resulting from the injury. PRC is mostly a salvage operation but given the severity of ligamentous disruption, the need to restore the patient's mobility and also the fact, that scaphoid was irreducible, a proximal row carpectomy (PRC) was performed to preserve wrist range of motion (ROM). Patient medical history The 86-year-old patient crashed the car into the wall of his garage at a speed of 30 km/h. As a result, the patient presented a dislocation of the lunate bone and the scaphoid. The patient lived alone and was completely independent. Regarding other conditions, he suffered from arterial hypertension and prostate cancer. Before and After Patient examination There was a visible deformity at the right wrist with bruising, and swelling. Additionally, a positive Hoffman-Tinel sign was observed with paresthesia in the median nerve area. A radiological examination of the hand was then performed, which revealed a dislocation of the scaphoid and lunate bones. No bone fractures were detected. Pre-operative considerations Given the severity of ligamentous disruption and the need to restore the patient’s mobility a proximal row carpectomy (PRC) was performed to preserve wrist range of motion (ROM). 1 Surgical Dorsal Exposure The surgical procedure involved exposing and splitting the 4th and 3rd extensor tendon compartments to facilitate access. The extensor pollicis longus (EPL) tend

Case 16: Utilizing the reverse radial forearm flap for burn wound management of the hypothenar part of hand
David Salim, MD, Msc
Keywords: Reverse radial forearm flap, Burn wound management, Hand surgery Authors: David Salim, MD and Taiba Alrasheed, MD, FRCSC, Msc. Institution: Department of Plastic- & Breast Surgery , Zealand University Hospital Roskilde, Denmark Abstract A 55-year-old man had sought and was admitted to the emergency department one week after sustaining a superficial second degree burn wound on the hypothenar region of the right hand after accidentally placing it on a hot stove. At first sight, the burn wound seemed quite superficial and conservative healing and bandaging was initially deemed sufficient with the aim of spontaneous healing. One week after the initial assessment in the emergency department, the patient was seen for a routine clinical control of the wound. At this consultation, the patient scored 4/4 positive Kanavel’s signs and flexor tenosynovitis was suspected. Afterwards immediate wound revision of the right hypothenar was conducted. During wound revision, considerable amounts pus was noted and furthermore the musculus abductor digiti minimi was avital and excised. Suitable wound dressing was applied, pus was sent for culture and sensitivity testing and the patient was gives appropriate peroral antibiotics. After numerous wound revisions and debridement, control of the infection at the orthopedic surgery department was achieved. The patient was then referred to the plastic surgery department for planning of soft tissue coverage with a reverse radial forearm flap. Patient medical history The patient was known to have substantial unregulated diabetes mellitus type two, but no other known medical comorbidities. Before and After Patient examination The patient was seen in an outpatient setting in the plastic surgery department for planning of surgery. The defect was located to the whole hypothenar region of the right hand. Substantial soft tissue loss was noted and the 3-5th flexor tendons were exposed. Pre-operative considerations A reverse radial forearm

Case 15: Closure of a complex defect after a dog bite wound of the middle third of the face
Dr. Guillermo Alvarez-Sanchez, Ignacio Lugo-Beltran
Keywords: Cheek reconstruction, face, cheek, forearm, free flap, Neurorrhaphy , radial forearm flap Authors: Dr. Guillermo Alvarez-Sanchez, MD ; Ignacio Lugo-Beltran, MD, Chief, Dr. Haro-Cruz Jorge Said, MD. Institution: Plastic and Reconstructive Surgery Division of Microsurgery, Hospital Angeles Metropolitano, Cuauhtémoc, Mexico. Abstract A 52 year old female who presents to the emergency room after receiving a dog bite in her right face, the defect is managed with a free radial forearm flap. Patient medical history 52 year old female, without past medical history, presented to the emergency room, referring she was attacked by her dog at her house, suffering a bite on her right cheek, with bleeding and loss of skin Before and After 1 Before photo - Arrival at the ER Facial asymmetry, with a complex wound on the right cheek, with skin loss, a defect approximately 10 x 9 cm, irregular borders, with muscle exposure, visualizing blood vessels and section of the buccal and zygomatic terminal nerve branches, active mild bleeding. Intact parotid gland and Stensen duct. Laceration of the zygomatic ligament. Difficulty mobilizing of the zygomatic and buccal branches muscle groups. Patient examination Facial asymmetry, with a complex wound on the right cheek, with skin loss, a defect approximately 10 x 9 cm, irregular borders, with muscle exposure, visualizing blood vessels and section of the buccal and zygomatic terminal nerve branches, active mild bleeding. Intact parotid gland and Stensen duct. Laceration of the zygomatic ligament. Difficulty mobilizing of the zygomatic and buccal branches muscle groups. Pre-operative considerations Given the circumstance of tissue loss, active bleeding and section of the nerve branches, also being a contaminated wound, we decided to go to the operating room immediately Due to tissue loss dimensions, we planned a radial free flap for tissue coverage 2 Debridement and assessing damages we cleansed, remodeled the irregular borders and clos
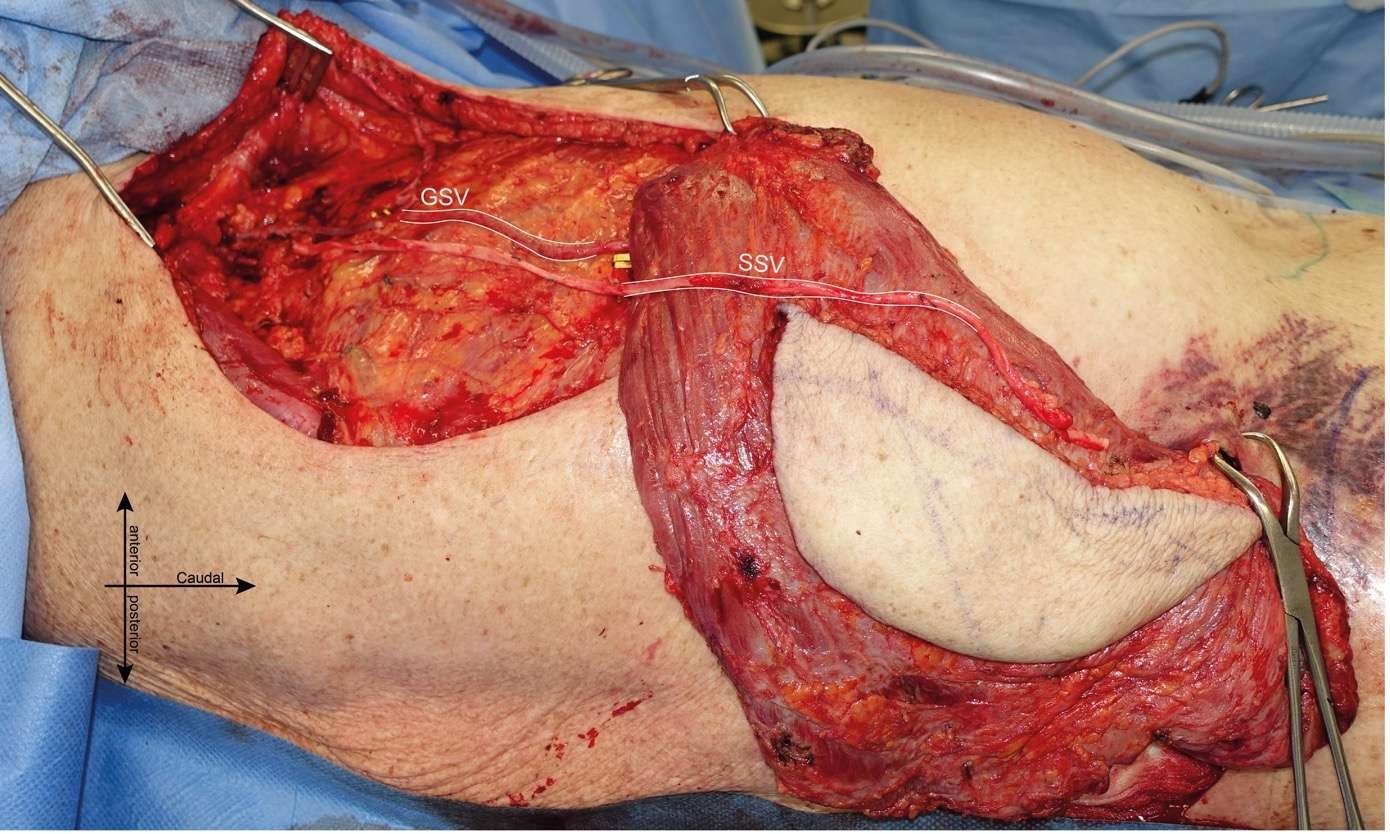
Case 14: Pushing Beyond Anatomical Boundaries: Latissimus Dorsi Sliding Flap for Lower Thoracic Wall Reconstruction
Sophie Osenegg, Oliver Didzun, Amir K. Bigdeli, Chief
Keywords: Latissimus dorsi flap, sliding flap, thoracic wall reconstruction Authors: Sophie Osenegg, MD, Oliver Didzun, MD, Amir K. Bigdeli, MD, Chief. Institution: Department of Plastic, Reconstructive, Aesthetic and Hand Surgery, Klinikum Kassel, Teaching Hospital of Philipps University Marburg, Kassel, Germany Abstract A 78-year-old multimorbid patient with chronic osteomyelitis and a full-thickness soft tissue defect (12 × 6 × 5 cm) of the right flank required flap reconstruction following multiple debridements. Given the absence of nearby recipient vessels and perforators, an ipsilateral myocutaneous latissimus dorsi sliding flap was selected. The thoracodorsal pedicle was extended by 30 cm using autologous venous grafts to achieve cranial reach while preserving anterograde arterial flow. This case illustrates the rarely described use of a latissimus dorsi sliding flap in complex reconstructions, emphasizing vascular adaptation techniques. Patient medical history A 78-year-old male had undergone right-sided nephrectomy in 1970 for renal cell carcinoma. Following initially uneventful wound healing, a chronic wound developed at the nephrectomy site, which the patient managed conservatively over the subsequent decades. In September 2024, he presented with spontaneous purulent discharge from the right flank, attributable to chronic osteomyelitis of the adjacent ribs. In addition, intraperitoneal infection with Staphylococcus aureus was confirmed. Serial debridements were performed by the departments of general and thoracic surgery, including partial rib resections and an atypical laparotomy. These interventions resulted in a full-thickness soft tissue defect of the right flank, measuring 12 × 6 × 5 cm, with exposed ribs and peritoneum. The patient was subsequently referred to our department for reconstructive management under ongoing open wound therapy. At the time of presentation, his medical history included stage V chronic kidney disease with initiation of hemod

Case 13: Advancing Nasal Ala Reconstruction: Novel Single-Stage Bullhorn Flaps vs. Traditional Two-Stage Nasolabial Techniques
Lukas Kure-Rosenberg, Nicco Krezdorn, Chief
Keywords: ala nasi, nasolabial flap, infranasal flap, bullhorn modification, facial reconstruction Authors: Lukas Kure-Rosenberg, MD, Nicco Krezdorn, MD, Chief. Institution: Department of Plastic & Breast Surgery, Zealand University Hospital, Denmark Abstract Reconstructive surgery of the caudal ala nasi poses a particular challenge due to the complex anatomy and high aesthetic significance of the area. The skin in this region is thick, inelastic, and poorly mobile, and the alar contour plays a crucial role in the overall symmetry and three-dimensional shape of the nose. Additionally, local tissue availability is limited, making flap design and execution technically demanding. Two-stage procedures, which are often required in this area, can be disadvantageous as they involve prolonged treatment time, multiple interventions, and temporary aesthetic or functional compromise between stages, potentially affecting patient satisfaction. Preoperative considerations should include a detailed assessment of the defect’s size, depth, and proximity to the alar rim, as well as evaluation of nasal symmetry, skin quality, and patient expectations. It is also important to plan for structural support, such as cartilage grafts, if there is a risk of alar collapse or distortion. This report presents three cases involving patients treated for basal cell carcinoma (BCC) on the caudal part of the nasal ala, following excision with frozen section guidance. Case 1 underwent a traditional two-stage nasolabial flap and demonstrated the subsequent need for revision due to dynamic tension and functional concerns. Case 2 introduces a novel single-stage, medially based infranasal flap – a "modified half bullhorn approach" – tailored to address smaller defects in a single-stage, cosmetically discreet and functionally balanced manner. Case 3 introduces an even larger single-stage, medially based contralateral bullhorn transposition flap with advancement closure – a "modified full bullhorn appr

Case 12: Flower Flap - A Novel Papilla Reconstruction Technique Using Local Flaps and Skin Graft
Anna Louise Norling, Nanja Gotland Sundstrup, Matilda Svenning Hunt
Keywords: Flower Flap, Papilla reconstruction, nipple reconstruction, breast revision, full-thickness skin graft, dog ear correction Authors: Anna Louise Norling, MD, Nanja Gotland Sundstrup, MD, Matilda Svenning Hunt, MD and Pia Cajsa Leth Andersen, MD. Institution: Department of Plastic Surgery and Burns, Rigshospitalet, Copenhagen University Hospital, Denmark Abstract A 47-year-old woman underwent bilateral papillae reconstruction using a novel reconstruction technique involving four local flaps and a full-thickness skin graft including subcutaneous tissue from excised dog ears, due to scar correction, following a DIEP flap breast reconstruction. This technique preserved breast projection, avoided additional scarring, and improved breast contour. Initial epidermolysis occurred, as expected with a thick graft, but the grafts survived. At one month follow-up, the papillae showed resolving discoloration. This simple and reliable method facilitates simultaneous nipple reconstruction and aesthetic breast contouring with minimal donor-site morbidity. Patient medical history A 47-year-old woman with a history of DCIS in the left breast and a family history of breast cancer (BRCA-negative) initially underwent bilateral subcutaneous mastectomy with NAC removal and implant-based reconstruction in 2021. Due to dissatisfaction with the result, she had bilateral DIEP flap reconstruction in May 2023. In July 2024, a revision was performed to improve the breast shape, including correction of dog ears and redundant skin on the DIEP flaps, as well as lateral liposuction. At the 3-month follow-up, the breasts remained laterally full with a square appearance. A new revision was planned to refine the contour and simultaneously reconstruct the nipple using a novel technique combining four small local flaps and a full-thickness skin graft with subcutaneous tissue. Before and After Patient examination The patient was a well-preserved woman with good-quality skin. Clinical examination r
Case 11: Closure of a larger defect on the cheek with the versatile bilobed flap
Sahar Vanessa Amiri (MD) and Matilda Svenning Hunt (MD)
Keywords: bilobed flap, larger facial skin defects, cheek reconstruction, reconstructive surgery Authors: Sahar Vanessa Amiri (MD) and Matilda Svenning Hunt (MD). Institution: Department of Plastic Surgery and Burns, Rigshospitalet, Denmark Abstract This case describes the use of a bilobed flap for reconstruction of a large cheek defect following excision of a squamous cell carcinoma in an 86-year-old male. Due to the tumor size and previous surgical scarring, direct closure was not feasible. The bilobed flap was chosen as the preferred reconstructive approach because of its ability to provide adequate coverage of the defect while allowing for primary closure of the donor site. Postoperative follow-up at three months demonstrated satisfactory aesthetic outcomes, with no wound complications or recurrence. Patient medical history The patient, an 86-year-old male diagnosed with hypertension, paroxysmal heart flutter, and with a history of carcinoma, was referred to us with a large, localized tumor on the right cheek. According to the patient's history, the tumor had been present for more than one year. The biopsy showed squamous cell carcinoma, and the histological subtype was unspecified. On clinical examination, the tumor was described as 20*25*6 mm, localized on the parotid gland, and clinically not adherent to the underlying tissue. The patient had a scar from a previous full-thickness skin graft (FTSG) on the right temple. There were no palpable regional lymph nodes. The patient was operated on under local anesthesia. Because of the size of the tumor, direct closure was not feasible. Local flaps were deemed a preferred reconstruction method. The tumor was excised with a 7 mm safety margin and depth excision margin to SMAS (Superficial Musculoaponeurotic System). Histology from frozen sections showed no malignancy. Before and After Patient examination The patient presented with significant sun damage and poor skin quality. The tumor was 20 x 25 mm in diameter and e
Case 10: Plication of rectus diastasis 2 years after twin-birth
Theresia Skytte Eriksen, Helle Sjøstrand and Ida Felbo Pold
Keywords: Rectus Diastasis, Plication, Abdominoplasty, following pregnancy Authors: Theresia Skytte Eriksen, Helle Sjøstrand and Ida Felbo Pold. Institution: Department of Plastic Surgery, Herlev and Gentofte Hospital, Denmark Abstract 38-year-old woman underwent plication of symptomatic diastasis of the rectus abdominal muscles after twin-birth by caesarean section. The diastasis had a maximal width of 6,6 cm just above the umbilicus and her symptoms included core-instability, back-pain, and a feeling of being unprotected around her abdomen especially while handling her children. Patient medical history 38-year-old woman had after twin-birth developed symptomatic diastasis of the rectus abdominal muscles. She had no comorbidities. She had an older child of 6 years, and the twins were 2 years old. All children were delivered by uncomplicated caesarean section. The patient described symptoms as back-pain, nausea, core instability, discomfort during running, and pain when encountering pressure to the abdomen especially while handling the children. Physical rehabilitation with physiotherapists had not been successful and hard to complete do to discomfort and pain. Before and After Patient examination The patient was initially examined 15 months postpartum and at an additionally examination two years postpartum by the same surgeon. A preoperative CT-scan at 15 months postpartum, showed a rectus diastasis with the maximal width of 6,6 cm just above the umbilicus. The objective examination confirmed those findings, and a small umbillical hernia was detected. No change in symptoms and width of the diastasis was found between the two examinations. Pre-operative considerations Physical training alone has not been found to reduce the width of the diastasis [1]. Surgery was in one randomized controlled trial superior to physical training with regard to reduction of pain and increase abdominal muscle strength [2]. The swedish guidelines currently recommend that surgery is indic

Case 9: Adipofascial Turnover Flap for Reconstruction of a Dorsal Finger Defect Following SCC Excision
Lukas Kure-Rosenberg, MD Nicco Krezdorn, Chief
Keywords: Squamous cell carcinoma, adipofascial, turnover flap, finger, defect, reconstruction Authors: Lukas Kure-Rosenberg, MD Magnus Balslev Avnstorp, MD Nicco Krezdorn, MD, Chief. Institution: Department of Plastic Surgery, Zealand University Hospital, Denmark Abstract Reconstruction of finger defects presents unique challenges, particularly in those with complex anatomical involvement. We present a case involving an immunosuppressed patient with a larger late diagnosed SCC, the excision of- and subsequent reconstruction- utilizing an adipofascial turnover flap (APTF), that offers a reliable and versatile option for addressing these challenges, while preserving hand function and aesthetics. A 74-year-old male with a history of kidney transplantation and long-standing immunosuppressive therapy presented with a highly differentiated SCC on the dorsum of the right fourth finger. The lesion, measuring 40 × 35 mm, extended to the proximal and distal interphalangeal joints. Surgical management included two stages: tumor excision with clear margins, followed by secondary reconstruction utilizing an APTF combined with a split-thickness skin graft (STSG). Preoperative and perioperative Doppler assessments guided flap design and ensured adequate vascularity. The APTF provided robust soft-tissue coverage of the exposed extensor tendon, with adequate perfusion confirmed by Doppler. The STSG demonstrated partial take but effectively covered the underlying APTF. Postoperative assessments were followed 30, 48, and 106 days postoperatively. Range of motion (ROM) showed postoperatively some limitations in the affected finger, particularly in the PIP and DIP joints, but functionality was aimed preserved with ongoing therapy. We demonstrate in this clinical case, how APTF is an effective and versatile reconstructive option for complex dorsal finger defects. Its robust vascular supply, adaptability, and minimal donor site morbidity make it particularly advantageous in immunosuppres

Case 8: Perialar Crescentic Advancement Flap for Nasal Reconstruction
Lukas Kure-Rosenberg, MD, Chief
Keywords: Nasal reconstruction, perialar flap, crescentic, advancement, PCC in situ. Authors: Lukas Kure-Rosenberg, MD and Nicco Krezdorn, MD, Chief. Institution: Department of Plastic Surgery, Zealand University Hospital, Denmark. Abstract We present the case of a 68-year-old woman with a residual PCC in situ on the nasal dorsum following initial excision and open defect by colleague. The initial pathology revealed incompletely excised changes cranial to the primary defect (12 o’clock position). The patient was booked for re-excision and closure, originally planned with a full-thickness skin graft (FTSG). However, the patient expressed high cosmetic expectations, prompting a change in plan to a local flap-based reconstruction. A perialar crescentic advancement flap was chosen, utilizing the planned re-excision site, which anatomically corresponded to a burrow triangle in the flap design. This case illustrates how integrating oncologic and reconstructive planning can optimize both margin control and aesthetic outcomes. Patient medical history A 68-year-old woman was referred for further management of an ulcerating lesion, consistent with biopsy-confirmed squamous cell carcinoma (SCC/PCC) in situ on the nasal dorsum. The patient was routinely seen at dermatological checkups due to being kidney transplanted, and was therefore also recommended surgical management of the lesion. The lesion was initially excised by a colleague and left as an open wound for secondary intention until the final pathological analysis. Pathology demonstrated no invasive tumor, but histopathological evaluation revealed residual SCC in situ/atypical changes at the superior (12 o'clock) margin of the excised area, necessitating re-excision. Before and After Patient examination Upon reexamination, the surgical defect was located centrally on the nasal dorsum, cranial to the supratip area, measuring 12 mm in diameter. The previously excised region had demarcated edges and healthy granulation tissu

Case 7: Cervicofacial Flap for Cheek Reconstruction Post Excision of Pigmented Solid Basal Cell Carcinoma
Bertha Kawilarang, Agus Roy Rusly Hariantana Hamid, I Gusti Putu Hendra Sanjaya
Keywords: cervicofacial flap, reconstruction, basal cell carcinoma, facial, cheek Authors: Bertha Kawilarang, MD, Agus Roy Rusly Hariantana Hamid, MD, I Gusti Putu Hendra Sanjaya, MD. Institution: Department of Plastic Reconstructive and Aesthetic Surgery. Prof. dr. I.G.N.G. Ngoerah General Hospital, Bali, Indonesia Abstract Background: Basal cell carcinoma (BCC) is the most common skin malignancy, with the pigmented solid subtype being a rare variant. Surgical excision with clear margins remains the mainstay of treatment, but reconstruction of facial defects requires careful planning to optimize both function and aesthetics. Case Presentation: We report a case of a 59-year-old female with a pigmented solid BCC of the right cheek. Wide local excision was performed, achieving histopathologically confirmed clear margins. The resultant defect, extending from the midface toward the nasolabial fold, was reconstructed using a cervicofacial advancement-rotation flap. Novelty and Rationale: The cervicofacial flap was selected due to its robust vascularity, excellent tissue match, and ability to provide a tension-free closure with minimal donor site morbidity. The flap was elevated in a subcutaneous and sub-SMAS plane to preserve vascularity, primarily based on the perforators from the facial and transverse cervical arteries. Meticulous dissection in the preauricular and cervical regions allowed for optimal mobilization without compromising facial nerve integrity. A lateral undermining technique enhanced flap rotation and reduced standing cutaneous deformities, ensuring a natural contour. Outcome: The patient’s postoperative course was uneventful, with complete flap survival and no complications. At the 6-month follow-up, there was no evidence of tumor recurrence, and the patient expressed high satisfaction with the functional and aesthetic results. Conclusion: This case highlights the cervicofacial flap as a versatile and reliable option for large cheek defects following on

Case 6: Fingertip reconstruction by a V-Y flap and eponychial flap in a patient with fingertip amputation
Alina Strohmaier, Martina Greminger
Keywords: Fingertip amputation; hand trauma; local flap; eponychial flap; V-Y flap Authors: Alina Strohmaier, MD, Martina Greminger, MD. Institution: HOCH Cantonal Hospital St. Gallen, Switzerland Abstract A 58-year-old male presented with fingertip amputation of the left index finger after a bicycle accident. The injury was classified as Ishikawa Zone 2/Allen Type III, with ulnar oblique pulp defect, subtotal nail bed loss but with intact germinative matrix, and exposed bone. Treatment involved a volar V-Y advancement flap for soft tissue coverage and an eponychial flap to allow visible nail growth. Postoperatively, early mobilization was conducted. At 6-month follow-up, the patient reported good functional outcomes. Examination revealed adequate soft tissue coverage, a normally growing but short nail without a claw-nail deformity, and a stable fingertip. The patient was able to play the piano again. A near-complete range of motion and normal sensation were achieved. This case demonstrates successful fingertip reconstruction using local flaps to restore function and maintain the nail, even when the nail bed is almost completely injured. Patient medical history A 58-year-old male patient presented to the emergency department with amputation of the distal phalanx of the second digit on the left dominant hand. The patient sustained the injury while inspecting the brakes of a bicycle, resulting in the second digit impacting the bicycle spoke. The patient is a professional piano player. No regular intake of medication. Before and After Patient examination Emergency presentation of the patient with fingertip amputation (Ishikawa zone 2, Allen Type III) of the left index finger. Initial examination revealed an ulnar oblique amputation of the distal phalanx of the index finger (adominant). The visible part of the nail bed was almost completely injured; however, the germinative matrix remained intact. Sensitivity and blood circulation were preserved. Tendon function was int

Case 5: Hatchet flap for reconstruction of a defect on the anterior chest wall
Carolina Maria Helena Hilton, Magnus Balslev Avnstorp
Keywords: Hatchet flap, thoracic skin defect, malignant melanoma, reconstruction Authors: Carolina Maria Helena Hilton, MD, Magnus Balslev Avnstorp, MD. Institution: Department of Plastic & Breast Surgery, Zealand University Hospital, Denmark Abstract A 73-year-old man was diagnosed with a malignant melanoma on the left anterior chest wall. According to guidelines he was scheduled for re-excision in 20 mm and sentinel node procedure. The defect following re-excision was too large for primary closure. A Hatchet flap was designed, covering the defect, with a cosmetic and functionally acceptable result. Patient medical history A 73-year-old man with a past medical history including hypercholesterolemia, hypertension, coronary stent and multiple earlier skin cancers (non-malignant-melanomas) was referred to the Plastic Surgery Department at Zealand University Hospital, Denmark, with a suspicion of malignant melanoma located on the anterior left chest wall. The tumor was excised with a 5-mm excision margin according to Danish guidelines (from “Dansk Melanom Gruppe” (the Danish Melanoma Group)). Histology showed a 1,9 mm thick malignant melanoma. The initial excision of 5 mm was not radical. The patient was therefore, according to Danish guidelines, planned for re-excision of 20 mm to the muscle fascia and closure with a local flap and sentinel node procedure. Before and After Patient examination The skin examination showed a cicatrice on the left chest wall, close to the neck, measuring around 30 mm, where skin mobility was not sufficient for direct closure if excised with a 20 mm margin. A lymph node scintigraphy showed two sentinel nodes in the left axilla. The patient was taking acetylsalicylic acid which was continued according to Danish guidelines (from “Dansk selskab for Trombose og Haemostase” (the Danish society of Thrombosis and Hemostasis)) . Pre-operative considerations Direct closure would probably result in reduced neck mobility or at least uncomfortable

Case 4: Unmasking the Decollement: Timely and Successful Primary Full-Thickness Skin Grafting in Complex Lower Leg Trauma
Laura Emilie Marr Spore, Claes Hannibal Kiilerich
Keywords: Decollement injury, full-thickness skin graft, primary full-thickness skin grafting, lower leg trauma, soft tissue debridement, perforating blood supply, atypical decollement, plastic surgery, trauma management, diabetes, case report Authors: Laura Emilie Marr Spore, MD., Claes Hannibal Kiilerich, MD. Institution: Department of Orthopedic Surgery, Holbæk Hospital, Denmark Abstract An 84-year-old female sustained significant lower leg trauma after a fall on a staircase. Intraoperative evaluation revealed a decollement injury. Defined as separation of the skin and subcutaneous tissue, from the underlying fascia, separating the perforating blood vessels from the subcutaneous tissue—with the affected skin area destined for necrosis, if not acted upon. Prompt debridement and primary full-thickness skin grafting of the affected skin were performed within hours. Early recognition and management are often needed, to avoid devastating injuries. This case highlights a successful treatment, and the need to focus on these injuries, as no clinical guidelines exist. Patient medical history The patient, with a history of type 2 diabetes, CKD 5 (Cronic Kidney Disease Stage 5, eGFR < 10, weekly dialysis) and poor skin quality, experienced a fall from standing height on a stone staircase. These factors contributed to a complex decollement injury despite the low-energy trauma. She hit the staircase corresponding to her tibial tuberosity, and a grinding motion during the fall resulted in the visual distal open lesion — only a small proximal wound suggesting where she struck the stairs initially, where the decollement lesion was later discovered to be starting from. The decollement injury is most commenly seen in victims in severe traffic accidents and typically involves opposing, intense forces that tear the skin and the subcutaneous layer away from the underlying fascia, thereby compromising the blood supply to the skin. And is often underdiagnozed and hard to recognize.

Case 3: Rieger-Marchac Dorsal Nasal Flap Revisited: An Old But Versatile Flap for Nasal Reconstruction
Pavitra Ramasamy, Koh Khai Luen, Mohammad Ali Mat Zain, Wan Azman Wan Sulaiman
Keywords: Nasal reconstruction, plastic, surgery, tumor reconstruction, rieger-marchac Authors: Pavitra Ramasamy, Koh Khai Luen, Mohammad Ali Mat Zain, Wan Azman Wan Sulaiman. Institution: Universiti Sains, Malaysia Abstract Reconstructing the nasal tip and lower third defects after neoplasm excision is challenging due to the nose’s complex structure. We present an 82-year-old man with basal cell carcinoma at the nasal tip-alar junction. Following surgical excision with a 3mm margin, the full-thickness defect was reconstructed using the Rieger-Marchac dorsal nasal flap. This technique effectively restores nasal form and function while ensuring optimal aesthetic outcomes, making it a reliable approach for nasal defect repair. Patient medical history Hypertension, diabetic mellitus, bronchial asthma, recent history of burrhole and drainage of subdural haemorrhage post fall and chronic smoker. Before and After Patient examination He presented with hyperpigmented lesions at the junction between nasal tip and the right alar of the nose for more than 10 years. It was initially a small mole like lesion which increase in size progressively in past 1 year. It was also associated with contact bleeding (Figure 1). The 2.0 x 2.0cm infiltrative, pearly lesion extended from right nasal supratip to the right alar groove. No evidence of transnasal involvement however ulceration was observed Pre-operative considerations Patient evaluation includes medical history to assess comorbidities like smoking that may affect healing Confirm complete tumor excision with frozen section or histopathology Consider nasal symmetry, contour and airway patency which may affect the functional concerns The defect need to be evaluated. Typically used for detects on the nasal septum, tip or sidewalls, need to consider adjacent tissue laxity for optimal flap mobilization Surgical planning of flap design on the superiorly based dorsal nasal flap consideration tension and vascularity and assess how to closu

Case 2 - 2025: Reconstruction of an extensive foot defect using a combined sensory split latissimus dorsi and serratus anterior muscle flap
Dr. med. Luisa Lotter, PD
Keywords: Lower extremity; Flap; Reconstruction; Soft tissue; Trauma; Microsurgery; Foot; Latissimus Dorsi ; Authors: Dr. med. Luisa Lotter, Dr. med. Ilja Käch, PD Dr. med. Volker Schmidt. Institution: Kantonsspital St. Gallen, Switzerland Abstract A 67-year-old male patient sustained a complex foot injury with an open Lisfranc dislocation of the medial cuneiform bone and shaft fractures of the 2nd to 4th metatarsals in July 2024, as a result of a crush trauma. After initial osteosynthetic treatment, a pronounced necrosis developed in the area of the hindfoot and forefoot over time and an implant-associated wound infection. The patient was then transferred to our tertiary care hospital for specialized defect reconstruction. At first radical necrosectomy was performed, resulting in a 10 x 12 cm soft-tissue defect in the heel area, which extended medially and laterally. In the area of the forefoot, there was also a full-thickness wound measuring 4 x 3 cm with exposed osteosynthetic material, bone, and tendon. Patient medical history The patient has no pre-existing conditions. Blood tests on admission showed a blood glucose level and HbA1c value within the normal range. An angiography was performed, revealing a regular three-vessel supply to the affected lower right leg. Before and After Patient examination Upon admission to our hospital, on assessment, the 67-year-old male patient was in good general health with a slim nutritional status. On the heel area of the right foot was a 10 x 12 cm soft-tissue defect, which extended medially and laterally. In the area of the forefoot, there was also a full-thickness wound measuring 4 x 3 cm with exposed osteosynthetic material, bone, and tendon. Blood tests on admission showed a blood glucose level and HbA1c value within the normal range. An angiography was performed, revealing a regular three-vessel supply to the affected lower right leg. Pre-operative considerations The reconstruction of complex soft tissue injuries with exp

Case 1 - 2025: Lower back reconstruction with free ALT flap, free radial bridge flap and vein graft
Andrea Donfrancesco, Karolinska
Keywords: Double free flap, flap to flap, free radial bridge flap, radial conduit, vein graft, lower back defect. Authors: Andrea Donfrancesco, MD and Jenny Löfgren, MD, Karolinska University Hospital, Stockholm, Sweden Abstract A challenging case of midline mid-lower back defect is presented. The patient underwent previously vertebral chondrosarcoma resection, spine fixation and post-operative radiotherapy, and was re-operated 2 years after because of vertebral bone re-absorption and rupture of the previously done spinal fixation. The skin and soft tissue never healed and the patient had a 22 x 10 cm defect of the mid-lower back with exposed fixation material, exposed dura above the spinal cord, and radiotherapy damaged tissue around. No local reconstructive option was feasible. We reconstructed the defect with a free ALT, connected to a free radial bridge flap and a saphenous vein graft, hooked up to the thoracodorsal vessel, and a new spinal fixation was performed. Reconstruction was successful. Patient medical history The patient is previously healthy, has no past medical history. She developed a bulge on the back at T12 level. MRI and biopsy showed chondrosarkoma. She was operated at Karolinska University Hospital in May 2022 with sarkoma resection, spinal fixation T 10 to L3, primary skin closure, and post- operative radiotherapy. After 2 years the patient presented with osteoporotic reabsorption of bone, fusion/collapse of L1-L2, and rupture of a shaft of the previous fixation. The patient underwent again surgery by the spine surgeon at our hospital in July 2024 with extraction of the previously done fixation, and a new longer fixation was performed T5 to L5. Beacuse the soft tissues ware previously irradiated, a left pedicled muscle latissimus flap was performed to have better coverage of the upper potion of the defect. The wound ruptured and got infected, with expsure of the spinal fixation material; the patient received targeted IV antibiotics and the woun